
FHIR, OMOP, openEHR: The Right Tool for the Right Job in Healthcare IT

As healthcare becomes increasingly digital, the ability to store, share, and analyze health data is more critical than ever. But behind every EHR system, public health study, or digital health app lies a vital question: how is the data structured and standardized? This is where data standards like openEHR, OMOP, and FHIR come into play. Organizations getting started with FHIR often benefit from practical guidance on setup and integration, our FHIR services overview explains where to begin.
While often discussed together, these standards were built with different purposes and philosophies. FHIR prioritizes flexible, real-time data exchange across diverse systems. OMOP focuses on unifying healthcare data for large-scale research and analytics. openEHR offers a deeply structured model for storing lifelong health records with semantic integrity.
Understanding how these standards differ, and where they can work together, is essential for anyone involved in healthcare IT, research, or policy. This guide breaks down each standard's architecture, real-world use cases, limitations, and strengths. Whether you're building a national EHR, designing a health app, or analyzing population health trends, this article will help you choose the right tool for the job. For a deeper dive into how FHIR is implemented locally, see our article on Understanding FHIR Implementation Guides in Australia.
Quick Definitions
Standard | Purpose | Maintained by |
|---|---|---|
FHIR | Exchanging healthcare data through APIs | HL7 (Health Level Seven) |
OMOP | Structuring data for research and population health analytics | OHDSI (Observational Health Data Sciences and Informatics) |
openEHR | Modeling and storing rich clinical data for long-term EHRs | openEHR Foundation |
These clinical data standards help unify how patient information is exchanged, stored, and analyzed.
What is FHIR?
FHIR (Fast Healthcare Interoperability Resources) is a standard developed by HL7 that makes it easy to share healthcare data between systems using modern web technologies like JSON, XML, and REST APIs.
Key Features:
Resources - Modular data elements such as Patient, Observation, Condition, etc.
Designed for interoperability and real-time data exchange.
Supported by major healthcare vendors and government mandates.
Real-World Example:
Imagine a mobile app that allows a diabetic patient to view their glucose levels and medication schedule. This app can request data from a hospital's FHIR API to retrieve the patient’s latest lab results (e.g., Blood Glucose Observation resource) and prescriptions (e.g., MedicationRequest resource).
FHIR makes such app development straightforward and compliant with data exchange standards. Many apps leverage the FHIR healthcare API to access real-time patient data.
Limitations:
Less suited for analytics or long-term record storage.
Resource flexibility can lead to inconsistent implementations.
Not intended for semantically rich clinical modeling like openEHR.
FHIR focuses on interoperability by enabling different systems to communicate regardless of how their data is stored internally. FHIR could play a key role in enabling EHR data interoperability across hospital systems. It doesn’t impose a specific way of persisting data. Vendors can continue using proprietary models as long as they can convert to and from FHIR formats for communication. To explore how FHIR compares to its HL7 predecessors, check out our article on FHIR vs HL7. To explore real implementations and try sample requests, you can use our FHIR test server.
What is OMOP?
The Observational Medical Outcomes Partnership (OMOP) Common Data Model (CDM) is a standard developed by the OHDSI community for the harmonization of health data for research. The OMOP data model provides a harmonized structure for research-ready health data. Its goal is to enable large-scale analytics across multiple data sources.
OMOP standardizes not only the data structure but also the vocabularies (e.g., SNOMED, RxNorm, LOINC), allowing researchers to query different databases in a consistent way. Unlike FHIR or openEHR, OMOP is not meant for real-time clinical use, but for secondary use like population health studies, cohort identification, and drug safety analysis.
Key Features:
Relational schema optimized for large-scale SQL queries.
Uses standardized vocabularies like SNOMED CT, RxNorm, LOINC.
Enables federated research networks through tools like ATLAS.
Abstracts away EHR-specific data models to a research-friendly format.
Real-World Example:
A public health researcher wants to study the effect of a specific cholesterol medication on stroke outcomes. Using OMOP, data from hundreds of hospitals can be queried with a single SQL statement to identify patients, their prescriptions, and stroke-related diagnoses, making large-scale comparative effectiveness research possible.
Behind the scenes, this often requires transforming data from proprietary formats. Tools like our FHIR converter simplify that process by automatically mapping source data into compliant FHIR resources.
Limitations:
Requires heavy ETL pipelines to transform source data.
Not designed for real-time decision support or clinical systems.
Limited support for longitudinal and complex patient narratives.
OMOP is the right choice when the primary objective is research and analytics across large datasets. If you're working on public health surveillance, pharmacovigilance, or academic research that relies on harmonized, comparable datasets, OMOP's CDM offers a mature, community-supported framework that enables collaborative science at scale.
What is openEHR?
openEHR is both a specification and platform architecture for building rich, semantically structured, and lifelong EHRs. openEHR’s architecture supports vendor independence and long-term semantic consistency.
A core idea of openEHR is vendor independence. Any system that conforms to openEHR specifications can understand and exchange data with another, without data translation. It is built for data persistence, meaning it's ideal for storing the complete health history of patients.
Key Features:
Based on a two-level modeling approach:
Archetypes: Standard definitions for clinical concepts like blood pressure.
Templates: Specific combinations tailored to clinical workflows.
Versioning and audit trails support medico-legal requirements.
Ideal for vendor-neutral data storage.
Designed for semantics-first EHR construction.
Real-World Example:
A national health system wants to build a unified lifetime EHR that remains valid and structured for decades. It chooses openEHR because it can ensure semantic consistency across evolving systems and clinical domains. A physician records a diagnosis using an archetype shared across institutions, ensuring the data is interpretable and queryable later for care or research.
Limitations:
Steep learning curve and higher modeling complexity.
Less tooling and community support than FHIR.
Requires clinical modeling governance.
openEHR is oriented toward persistence, providing a common data model and standardized templates that can be shared and reused across systems. It allows true semantic interoperability without translation, assuming all systems use openEHR natively.
openEHR is a strong choice when your goal is to build a deeply structured, long-term EHR system that supports high-quality clinical modeling. It is especially powerful in environments requiring semantic consistency across time and providers, such as national health records, hospital networks, or complex care environments. If vendor neutrality, precise data modeling, and data reuse across clinical tools are priorities, openEHR is an excellent foundation.
Comparing at a Glance
Feature | FHIR | OMOP | openEHR |
|---|---|---|---|
Primary Use | Data exchange/interoperability | Research & analytics | Long-term EHR modeling |
Data Structure | Modular resources (e.g., Patient) | Tables with standard vocabularies | Archetypes/Templates (semantic models) |
Real-time Use | Yes | No | Yes |
Optimized for Research | Limited | Yes | Not primarily |
Customization | High (via profiles/extensions) | Limited (schema-bound) | High (via archetypes) |
Government Mandate | Frequently required | Optional | Rarely required |
Global Adoption | High | Medium | Growing |
Best For | Integration, apps, HIEs | Population-level research | National EHRs, hospital systems |
Example Scenario: Research on Rare Diseases
Suppose you want to study a rare disease that only occurs in 2–3 patients per hospital. You need to:
Aggregate data across 100+ hospitals.
Standardize terminology (e.g., ICD-10, SNOMED).
Run analytics on medication outcomes and disease progression.
If you’re building something similar, you can connect to our FHIR test server to experiment with real-world API calls.
Best Choice: OMOP
OMOP is the best choice for this scenario because it supports federated data analysis without the need to centralize sensitive patient data. With OMOP, each hospital can convert its clinical data into a standardized format using consistent vocabularies like SNOMED CT and RxNorm. This enables researchers to run the same analytical query across multiple institutions, significantly increasing the sample size and the validity of rare disease research. It allows for scalable, reproducible analytics that can inform real-world evidence generation and public health policy.
Example Scenario: App Integration with Real-Time Access
Imagine a company developing a fitness app that helps users manage chronic conditions like hypertension. The app needs to:
Access blood pressure readings from various hospital systems.
Display medication adherence data.
Best Choice: FHIR
FHIR is ideal in this situation because it provides a standardized, API-driven approach to accessing real-time healthcare data across different systems. By leveraging FHIR, the fitness app can connect securely with hospital systems to retrieve live blood pressure readings and medication adherence records, all formatted in a consistent and machine-readable structure. Furthermore, the SMART on FHIR framework enables user authentication and consent management, making the integration both seamless and compliant with privacy regulations. This makes FHIR a powerful enabler for patient-facing applications and digital health innovation.
Example Scenario: Building a National Health Record
Suppose a country wants to implement a national EHR system that stores complete clinical histories for all citizens over decades. This system must:
Preserve data semantics.
Support clinical decision support.
Allow extensibility without breaking compatibility.
Best Choice: openEHR
openEHR is the optimal solution for building national EHR systems due to its focus on semantic consistency, longevity, and medico-legal soundness of clinical data. With its archetype-based modeling, openEHR ensures that the meaning of clinical concepts is preserved across different regions and over time. Its support for versioning and audit trails aligns with legal and clinical governance requirements, and the ability to create region-specific templates enables localization without breaking interoperability. These features make openEHR uniquely suited for storing comprehensive, structured health records that need to remain useful and trustworthy for decades.
Can They Be Used Together?
Yes — in fact, many modern health systems combine all three:
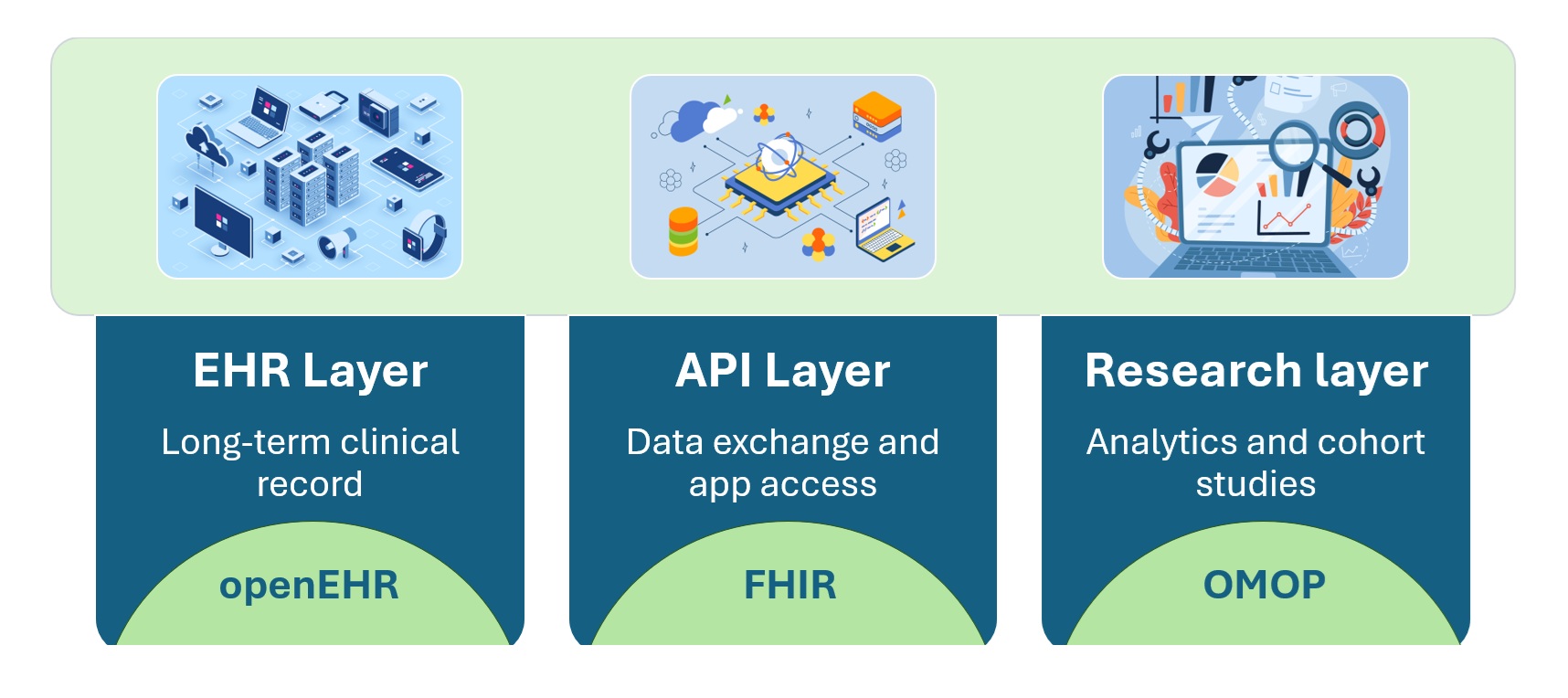
An example architecture:
Clinical data is entered into openEHR.
Exposed via FHIR APIs for third-party apps.
Periodically transformed into OMOP for research.
How to Choose
Choosing between openEHR, OMOP, and FHIR depends entirely on your project's needs. If your priority is to ensure seamless interoperability between healthcare systems, applications, and regulatory compliance, FHIR is the right standard due to its API-first, widely supported design. Our FHIR consulting and services provide the frameworks and accelerators to make that interoperability a reality.
For healthcare organizations aiming to build structured, long-term electronic health records with deep clinical semantics and strong versioning support, openEHR is the best choice.
When the main objective is to enable large-scale population health analytics, retrospective studies, or collaborative research across institutions, OMOP shines with its standardized schema and vocabularies.
Additionally, if you are developing a national or regional health information exchange system, FHIR is often mandated by governments. For projects involving clinical decision support and legally sound, longitudinal records, openEHR offers unmatched robustness. Lastly, if your organization seeks to contribute to or benefit from global research communities like OHDSI, adopting OMOP is essential.
We’ve written more on how modern data strategies are breaking down barriers, see Unleashing Healthcare Data Silos for real-world implications.
Final Thoughts
FHIR, OMOP, and openEHR are not competitors — they are complementary tools designed for different jobs. Choosing the right one depends on what you're building:
Use openEHR when you need a robust foundation for storing and modeling clinical data.
Use FHIR when you want to build applications that exchange data with existing systems.
Use OMOP when your goal is research, population health, or multi-institutional data analysis.
Rather than choosing just one, many healthcare systems benefit from strategically combining these standards. When integrated wisely, they enable a future where healthcare data is not only connected and computable, but also reusable for improving care, research, and outcomes at scale.
Let your use case guide your decision, not just trends or mandates.
Healthcare App Development & FHIR Services
From planning to integration and maintenance,
we deliver healthcare app development and FHIR services
that work seamlessly together.